

Background:
CMML is a myelodysplastic/myeloproliferative overlap syndrome associated with persistent monocytosis. Previous studies have shown a characteristic phenotype of peripheral blood (PB) monocytes in CMML that may have diagnostic utility. There is expansion of the classical monocyte (Mo1) population (CD14+CD16-) with concomitant reduction in the intermediate (Mo2; CD14+16+) and non-classical (Mo3; CD14-16+) populations. It is unclear whether an increased Mo1 population or a reduced Mo2/Mo3 population is a better discriminator in detecting CMML by flow cytometry. Diagnostic thresholds for these populations have most often been established by comparison with normal donors using PB samples. The objective of this study was to determine the optimal cut-off limits for flow cytometric monocyte repartition (FMR) in bone marrow (BM) samples and to assess the diagnostic accuracy of this method in patients undergoing BM evaluation for other causes of monocytosis using a novel gating strategy.
Patients/Methods:
71 BM aspirates were analysed comprising 35 confirmed CMML (21 proliferative CMML , 14 dysplastic CMML), 13 other myeloid neoplasm (MN) disease controls and 23 normal bone marrow aspirates. The MN cohort was identified through local samples with a known peripheral blood monocytosis of ≥1.0x109 and peripheral blast count of <20% not fulfilling criteria for CMML. The MN cohort comprised of 4 cases of chronic myeloid leukaemia (CML), 2 cases of myelodysplasia/myeloproliferative neoplasm unspecified (MDS/MPN-U), two cases of atypical CML (aCML), 2 cases of primary myelofibrosis, 1 case of juvenile myelomonocytic leukaemia (JMML), 1 case of chronic neutrophilic leukaemia (CNL) and 1 case of therapy-related acute myeloid leukaemia (T-AML). The median age of CMML patients within our cohort was 74 years (range 44- 89 years) and 77% were male.
Stored flow cytometric data were reanalysed to assess monocyte subsets. After initial removal of doublets and non-cellular events, sequential gating selected a CD45+CD33bright population with low side scatter to select monocytes and exclude granulocytes. The lymphocyte gate as determined on the CD45 vs CD33 plot was used to establish a threshold for CD16 positivity. Immature double negative monocytes (CD14-CD16-) were excluded as in published gating strategies.
Results:
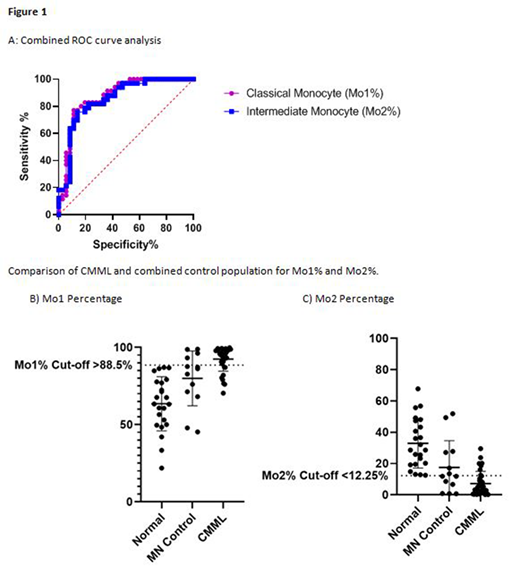
Linear regression analysis of the percentage of both the Mo1 and Mo2 populations demonstrated a significant difference between the CMML, MN, and normal cohorts (global P<0.0001). Post hoc analysis demonstrated a significant increase in the Mo1% fraction (mean 92.5%; 95% Confidence Interval [CI]: 88.1%, 96.9%) in CMML cases when compared to the normal BM cohort (mean 63.5%; 95% CI: 58.1%, 69.0%; comparison P <0.0001) and the MN cohort (mean 79.9%; 95% CI: 72.7%,87.2%; comparison P = 0.004). Conversely, the Mo2% was significantly decreased (mean 6.8% 95% CI: 2.7%, 10.9%) in CMML cases when compared to the normal cohort (mean 33.0%; 95% CI: 27.9%; 38.1%; comparison P value <0.0001) and the MN cohort (mean 17.6%; 95% CI 10.8%; 24.3%; comparison P value 0.008). Receiver Operator Curve (ROC) curve analysis of the Mo1 population demonstrated an area under the curve (AUC) of 0.8738 (95% CI: 0.7897, 0.9579; P<0.0001) with a marginally lower AUC for Mo2% (Figure 1A). Priority was given to selecting a cut-off value with higher specificity, considering that the BM examination is not a screening test. A cut-off value for Mo1% of >88.5% (Figure 1B) gave a sensitivity of 77.1% (95% CI: 60.98%, 87.93%) and specificity of 88.9% (95% CI: 74.69%, 95.59%) (Figure 1A). A Mo2% cut-off value of <12.25% (Figure 1C) gave a sensitivity of 78.8% (95% CI: 62.25%, 89.32%) with a specificity of 80.6% (95% CI: 64.97%, 90.25%) (Figure 1A). Eight patients with CMML were misclassified by the Mo1/Mo2 criteria.
Conclusion:
Our study confirms that analysis of monocyte subsets on BM samples provides good discrimination of CMML cases when compared to normal controls. There was significant overlap with other MN samples. FMR may be a useful adjunct to BM morphology in cases with subtle dysplasia. Further study is required to understand the overlap in monocyte phenotype between CMML and other myeloid neoplasms.
Allen:Amgen: Other: Travel Support; Roche: Other: Travel Support; Novartis: Other: Travel Support. Hahn:Roche: Honoraria; Astra Zeneca: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal